
SuCCeED IVC: Sustained Cancer Cell Energy Depletion
One dozen peer-reviewed articles* demonstrate how intravenous vitamin c selectively depletes energy from cancer cells, and when sustained over long-durations it results in Sustained Cancer Cell Energy Depletion (SuCCeED). This integrative therapy works differently than the typically fast-rate/short-duration intravenous vitamin c protocol, and ideally, should be combined with that protocol and other treatments that attack cancer directly. See “Potentiating Integrations”, below, for recommendations.
Extended Life by 4x for 100 patients, 40 Years Ago, But Was Too Expensive & Never Repeated
Though the moniker “SuCCeED IVC” is new, this strategy is not. Linus Pauling used this method 40+ years ago with 100 patients, all which were end-of-life on palliative care only. The treatment group lived 4 times longer on average compared to 100 controls who did not receive the treatment, and tumor response was so significant that caution is necessary with heavy tumor loads. Sadly, the protocol was very expensive in terms of manhours (all-day-long infusions, 5 days/week, over many weeks) so the protocol has never been repeated.
To make it more cost-effective the treatment administration rate increased dramatically thereafter. Treatment is now usually administered 30x faster and is done over a period of just 2-3 hours (instead of Pauling’s full week for the same dose). This is typically done 2x or 3x weekly, for as long as the patient can afford it.
Today we still use the super fast dosing method (relative to Pauling’s administration rate), but it has not demonstrated the cancer-killing power of Pauling’s long-duration protocol. Neither is today’s high-rate protocol compatible with all patients, and it comes with a number of contraindications as well as a few undesirable short-term side effects (see table below). Due to the original sustained slow-dose protocol, the original protocol would not have the same contraindications, neither would it have the same adverse side effects.
Mobile Pumps Make The Superior Method Very Affordable, More Compatible, and With Many Improvements
Mobile pumps (known as ambulatory pumps in the industry), are commonplace now especially for pain-relief following surgery, and are very easy to use> These pumps make the original sustained slow-dose protocol practical while providing many substantial improvements to the original 100-patient effort. These improvements include better dose consistency (0.5g/hour, all day long), duration (4-5 days uninterrupted), portability, and a vastly more affordable arrangement (because no hospitalization is required). The pumps also facilitate other factors including facilitating anti-hypoxia (oxygenating) aerobics to potentiate results, which is an essential part of the SuCCeED protocol (see Potentiating Integrations, below).
The table here demonstrates how SuCCeED complements conventional IVC (they work best together).
Comparison with Conventional IVC:
(FYI… Do both)
| Property |
Conventional IVC |
SuCCeED IVC |
| Rate | 40g/hr, +/- 20g | 0.5g/hr, +/- 1.5g |
| Duration | 90min, +/- 60 min | 7 days, +/- 3 days |
| Duration of cancer-killing effects | 6 hours | 7 days |
| Cytotoxic Mechanism | Multiple (incl. Energy Depletion) | Energy Depletion |
| Quality of Life Response | Excellent | Excellent |
| Facilitates concurrent synergistic aerobics | No | Yes |
| Req. Doctor Visits / Week | 2-3 | 1 |
| Outpatient Blood Ascorbate levels | Diminishes until reaches scurvy | Excellent |
| COMPATIBLE WITH PATIENTS WITH… | ||
| G6PD Deficiency | Can do Low-dose only | Compatible |
| Osmotic Issues (eg. Pulmonary Congestion) | A concern, require supervision | Compatible |
| Renal Insufficiency / Challenges | Not compatible | Decreases renal problems |
| Adrenal Insufficiency | Fix with cortisol | Compatible |
| Medium to High TLS Risks | Compatible | Possibly a risk |
| SIDE-EFFECTS | ||
| Fatigue | Sometimes | Always Invigorating |
| Vein Sclerosing | Possible | No problem |
| Tremors/Shakiness | Sometimes | No |
| Herxheimer | Sometimes | Decreases Herxheimer |
| Legend: | Excellent |
| Good |
SuCCeED More by Combining Methods
Ideally the patient combines the two methods. They can, for example, get the pump inserted at the same time as the large-dose (30g+ at a rate of 0.5 g/hr) infusion is started, either Monday or Tuesday, and then have it removed during another large-dose infusion, either Thursday or Friday.
A Note on Tumor Lysis
In the original Pauling protocol, the efficacy against tumors was so significant that a few of the patients experienced TLS, sadly resulting in death. For that reason, this protocol is currently not recommended for some patients as contraindicated in the bullet list below. Based on the original research done it is possible that this was an aberration since all 100 patients in the study were presumed end-of-life palliative care only and not expected to live more than a few days to a few months. Additional considerations: the exact administration rates of the original tests were never recorded, but the administration rates were adjusted manually, on the fly, resulting in likely large variances in blood ascorbates with respect to time. Mobile pumps normalize out those conditions due to the automatic dispersion of IVC fluid, and the administration rate can be reduced significantly over the Pauling trial if deemed beneficial.
Additionally, many advancements have taken place regarding risk-detection for TLS (See PMC4017246). A TLS assessment should be made for potential trial participants, and patients at medium to high risk for TLS are thereby excluded from use of this technology until the phenomenon can be studied further and ruled out as a contraindication for this protocol. This includes the following patients:
- patients with unusually heavy tumor loads
- acute lymphoblastic leukemia
- acute lymphocytic leukemia
- acute myeloid leukemia with white blood cell count > 50,000
- Burkitt’s lymphoma
- patients with compromised kidney function (cannot handle dead tumor debris)
- any 4 of the following (compared to baseline):
- 25% increase in uric acid
- 25% increase in potassium,
- 25% increase in phosphorus,
- 25% decrease in calcium,
- pretreatment creatinine concentration above 1.4 mg/dL
- 25% increase in lactate dehydrogenase,
- male gender
- splenomegaly (in hematologic malignancies)
There is a good likelihood that TLS can be managed by infusion rate for patients at high-risk, and it should be noted that TLS management has significantly improved since the original studies 40 years ago. Another possibility for these patients involves the use of AscorbylGlycine, which has a roughly 30% lower toxicity to tumors compared to sodium ascorbate, but these possibilities need more study before they can be tested in a clinical setting. Also, since conventional IVC has not demonstrated TLS and has demonstrated shrinking tumors, conventional IVC, as well as nano-sized liposomal C may be utilized to diminish tumor size to an acceptable level prior to engaging in the SuCCeED protocol.
For patients in the medium TLS risk (but not high), the above parameters can be closely monitored in real-time while receiving a very low rate (eg. 0.2g/hr), and if stable the rate can be tentatively increased as the practitioner deems prudent.
Vitamin C Protocol Comparison
The charts below demonstrate how the mobile pump protocols fit within the IVC ecosystem. It’s recommended that the SuCCeED protocol will be integrated with a protocol that attacks cancer directly, (such as conventional oncology, conventional IVC, liposomal C, and/or another treatment). When all indications of cancer have disappeared an additional course of the mobile pump, or with liposomal C (with true laboratory-validated nano-sized liposomes) is recommended. Thereafter a course of liposomal treatment for an additional 3-4 weeks is strongly encouraged. After remission, megadosing (pink line in the first chart) for many months is also strongly encouraged.
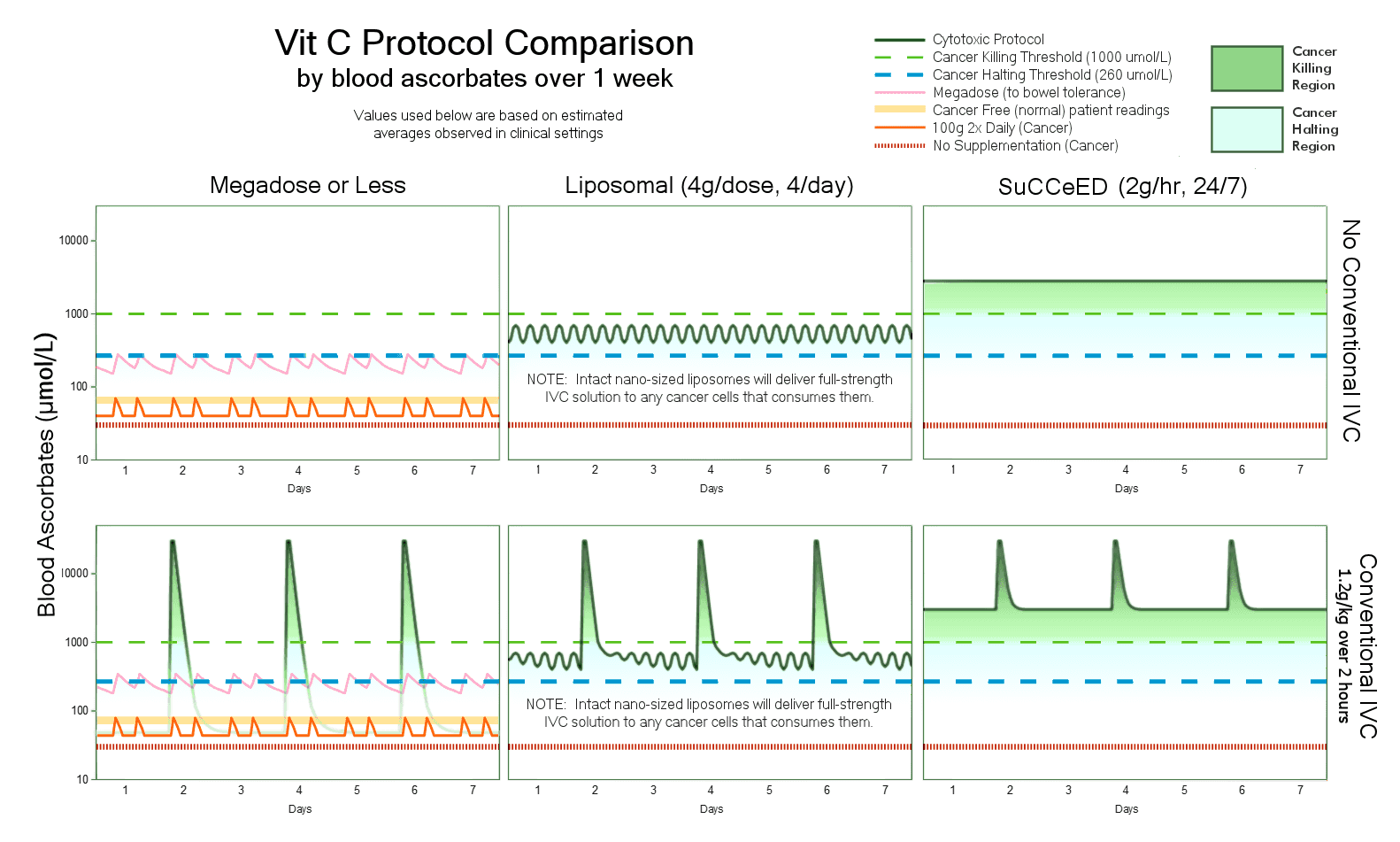
Note that the bottom right graph shows the most aggressive (and most promising) protocol combining both the conventional IVC approach (30+ grams, at 0.5g/min) combined with the SuCCeED protocol. They would receive the conventional IVC on Monday, and get the pump inserted as well, and then go in for another conventional IVC on Wednesday and Friday. During the Friday visit the pump would be removed. The patient would do this for this as many weeks as necessary to put the cancer into remission.
Potentiating Integrations:
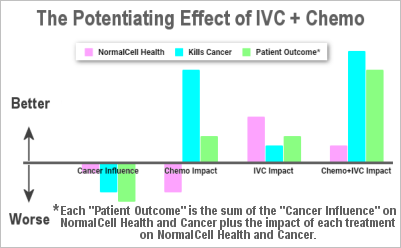
- Chemotherapy. All the studies with simultaneous IVC and chemo show a synergistic effect. (see 3.9a, 3.9b, 3.9c, 3.9d, 3.9e, 3.9f, 3.9g, 3.9h, 3.9i, 3.9j, 3.9k, 3.9l, 3.9m, 3.9n, 3.9o)
- Conventional Chemo
- Metronomic Chemo (similar to SuCCeED IVC, uses an all-day pump, but pumps minute amounts of conventional chemo)
- IPT Chemo
- Radiation Therapy (see synergistic effect: 3.10a, 3.10b, 3.10c)
- Aerobic Exercise to help oxygenate the hypoxic tumor areas and increase the IVC fluid to these areas. This is the #1 thing patients can do to increase efficacy and it is uniquely facilitated by the the use of a mobile pump.
- A diet of low carbs and low glycemic-index foods (also called “slow carbs”). Preferably, this should be mostly plant based (which is a challenge as so many of these diets are heavy on the animal products). Animal products are okay in moderation, moderation is the key. The combination of low-gi and low-carb prevents blood glucose from feeding cancer which would otherwise inhibit cancer death by NAD depletion.
- SuCCeED IVC potentiating supplements. See here for references.
- Artemisinin & Dfraction
- DCA (dichloroacetate)
- Quercetin
- Curcumin
- Alpha Lipoic Acid
- Vitamin E
- Vitamin K3, Vitamin K1 and K2
- Lecithin
- Doxycycline antibiotic. This also helps shut down the cancer cell energy process. Vitamin C shuts down the glycolic pathway, and doxycycline shuts down the OXPHOS pathway.
- Oxidative therapies. Hypoxia at the cancer site may be the #1 reason when treatment efficacy falls short of in vitro success predictions. Here are some mitigating strategies:
- Ozone
- UVBI
- O2 Mask
- Hyperbaric Oxygen
- DCA (dichloroacetate) administration
- Aerobic Exercise
References, and a quote (or quick summary) from each:
- Original long-duration protocol (50 patients):
http://www4.dr-rath-foundation.org/NHC/studien_pdf/old/the_orthomolecular_treatment_of_cancer.pdf - Addition information on the original 50 patients plus 50 patients:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC431183/pdf/pnas00040-0366.pdf - More information with a revised set of 100 patients (mostly the same patients):
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC336151/
Recent studies demonstrating cancer-cell energy depletion at mobile pump ascorbate doses:
- “vitamin C inhibited energy metabolism through NAD depletion, thereby inducing cancer cell death.” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4563566/
- ATP levels demonstrated a dose-dependent decline with ascorbate treatment. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2807999/
- “pharmacologic ascorbate concentrations diffuses into cells and mediates toxicity in sensitive cells by ATP depletion”. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1885574/
- “severely target energy production”: Vitamin C shuts down the glycolic pathway for cancer cell energy production. Combined with Doxycycline, which shuts down the OXPHOS pathway it demonstrated cancer cell energy depletion. 10.18632/oncotarget.18428
- Vitamin C causes NAD+ depletion (energy depletion), thereby inhibiting Cancer Stem Cell (CSC) activity exhibited by NADH expression, 10 times better than conventional methods. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5400535
- “ascorbate-induced oxidation … to decrease the ATP level in the cell”. https://www.ncbi.nlm.nih.gov/pubmed/12914777
- “inhibits GAPDH by both post-translational modifications and NAD+ depletion ultimately leading to an energetic crisis and cell death”. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4778961/
- “ascorbic acid concentrations produce extracellular H2O2, which can diffuse into cells, deplete ATP in sensitive cells, and thereby cause cell death”. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1885574/
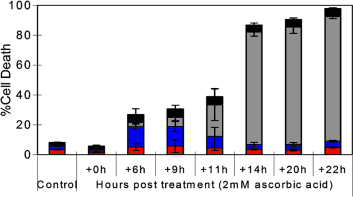
- See chart above, 2mM ascorbate dose takes at least 14 – 22 hours to fully starve cancer to death of energy (Note that it will be considerably longer in the human body due to hypoxic conditions). https://www.ncbi.nlm.nih.gov/pubmed/16157892
- “Practitioners should pay more attention to the cumulative vitamin C effect instead of the vitamin C concentrations”. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4031610/
Tumor Lysis Syndrome: New Challenges and Recent Advances
- F. Perry Wilson and Jeffrey S. Berns, Tumor Lysis Syndrome: New Challenges and Recent Advances, Adv Chronic Kidney Dis. 2014 Jan; 21(1): 18–26.
doi: 10.1053/j.ackd.2013.07.001 PMCID: PMC4017246 NIHMSID: NIHMS573366 - Aibek E. Mirrakhimov, Alaa M. Ali, Maliha Khan, and Aram Barbaryan, Tumor Lysis Syndrome in Solid Tumors: An up to Date Review of the Literature, Rare Tumors. 2014 May 13; 6(2): 5389 doi: 10.4081/rt.2014.5389 PMCID: PMC4083673